Police Chief Leonard Campanello’s New Fight Against the Heroin Crisis

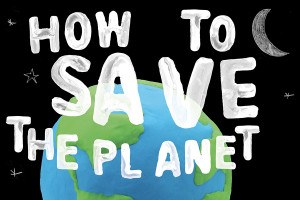
Volunteer Ruth Cote hugs a woman inside the police station in Gloucester, who has voluntarily come to the police for help kicking her heroin addiction. / AP Photo by Elise Amendola
Part of what made Campanello’s directive so revolutionary was that he claimed powers that the police, technically, do not have. His audacity did not go unchallenged. The Essex County district attorney, Jonathan Blodgett, wrote Campanello a letter pointing out that while his mission was laudable, police chiefs don’t have the legal authority to make “an explicit promise not to charge a person who unlawfully possess drugs.” The chief all but laughed at the missive, and ignored it. Some critics have asked what Campanello would do if someone came into his station house with 4 kilos of heroin and requested treatment—would he really not arrest them? I posed this hypothetical to him one afternoon. “What the fuck do I care?” Campanello fired back. “We’ll take the 4 kilos, get that off the street, and get the guy into treatment.”
Campanello is not the type to spend time mulling over hypothetical arguments. After all, hypothetical arguments won’t stop the flood of corpses washing up on his streets. As for the law? Well, as far as he’s concerned, the response to his edict—millions of hits on the original Facebook post, a stack of encouraging letters piled on his desk, a growing list of volunteers—amounts to an iron-clad mandate to end the war on drugs as we know it. Moreover, he’s convinced that if he can lay the groundwork for police to treat addiction as a health issue rather than a legal issue, other departments will follow en masse.
And there’s reason to believe that he’s right. Within weeks of Campanello launching his crusade, Walsh told reporters he was thinking about copying aspects of the program in Boston. A week after that, Massachusetts Attorney General Maura Healey gave Campanello a thumbs up: “We are not going to arrest or incarcerate our way out of this [epidemic],” she said. “This is a public health crisis and we must treat it and address it as such.” By August, the sentiment had somehow found its way into New Jersey Governor Chris Christie’s stump speech: Addiction, the Republican presidential candidate told a New Hampshire audience, “is a disease and the war on drugs has been a failure—well intentioned, but a failure.”
But Campanello isn’t content merely with changing our ideas about whether drug addicts are criminals—and he’s not satisfied with ending drug arrests. The fight he has in mind is much bigger than and almost as formidable as addiction itself. The real public enemies, in Chief Campanello’s world, are the insurance companies.
“The insurance system is set up for people to fail,” he says in a matter-of-fact manner that belies his disdain. “I think it comes down to money. I think it comes down to stigmatization. I think it comes down to the status quo.”
This is what the status quo looks like: Thirty-five miles southwest of Gloucester, an ambulance blasts down a quiet residential street in the city of Medford on a Friday night. A woman standing on the front porch of the house yells, “Get the Narcan!” when the crew steps out of the truck. Inside, splayed across the floor, is Mike, a lanky 22-year-old white guy with gray sweatpants and a shaved head who overdosed moments earlier. A paramedic administers a squeeze of aerosolized Narcan in each nostril, and within 90 seconds the young man returns from the brink.
Bewildered and drenched from a bucket of water his companions had dumped over his body in hopes of shocking him into consciousness, Mike (whose name has been changed to protect his privacy) trembles uncontrollably on the ride to Lawrence Memorial Hospital, his black Nike high-tops slapping together. He tells the paramedic that this is the first time he’s shot up since getting out of a rehab facility in Florida a week ago.
A few minutes after arriving at the hospital, Mike’s parents and their respective partners—his mom and dad split up when he was 17—barrel through the entrance. This is not unfamiliar territory for them. In fact, it’s frighteningly familiar. This is their son’s seventh overdose in two and a half years. As Mike’s father fights through tears of frustration and fear, the paramedic turns away and mentions how rare it is to see family members come to the hospital on an overdose call. Mike is calm and polite to the nurses, who strip away his soaked clothes and wheel his bed into a small alcove. His mom, Susan (whose name has been changed to protect her privacy), stands at his side, trembling with anxiety.
Mike grew up in a family that knows addiction well—one of his grandmothers drank herself to death by age 42, and his uncles, sisters, and father had struggles of their own. In high school, teachers caught Mike, never an A student, smoking pot, and he was subsequently expelled. Around this time he moved in with a relative and was introduced to the warm, body-tingling buzz of opioids by way of Percocet. Soon he was dependent, and he steadily ramped up his usage until the combination of curiosity and cravings pushed him to inject heroin for the first time at age 19. Then he overdosed, again and again.
Susan had to confront her son’s near-death injections in December 2014, when police found Mike unconscious behind the wheel of his car at a red light in Medford. They hauled Mike out of the vehicle, and an ambulance crew revived him with Narcan. Susan panicked when the officers told her Mike was being discharged into her custody, as he was not considered a danger to himself or anybody else. “How can you say that?” she pleaded. “He was just behind the wheel of a car, passed out, and you had to bring him back to life. He could have killed somebody.” Police issued him a citation for operating under the influence and possession of a Class A drug.
Mike needed treatment, but finding a bed was not easy. Susan called approximately 25 facilities around the state, and was told either that there was no room or that care wasn’t covered under MassHealth, the state-sponsored insurance coverage Mike had at the time. It took three days to find her son a bed in Danvers at a weeklong program, but only two days after dropping him off, Susan claims that the facility called her and told her that Mike was being discharged for allegedly writing on a bulletin board. Rules were rules, and it didn’t matter if Mike was going through withdrawal.
Before driving to Danvers to collect her son, Susan found a 30-day-long program in Florida that accepted his insurance with a hefty deductible. She arranged for him to fly down the same day, April 29, 2015, and booked the plane ticket. After a brief stop at home so Mike could pack his bags, they arrived at Logan. Susan didn’t know it, but Mike had heroin on him. Not long before takeoff, he went to the bathroom and overdosed. A medical team at the airport revived him, and an ambulance took him to Mass General. When they got home from the hospital, Susan rebooked Mike’s plane ticket for the first flight in the morning and barricaded herself in front of the door so he couldn’t sneak out of the house.
Mike spent a month in Florida before returning to Massachusetts in June. A week later, I met him for the first time in the back of the ambulance in Medford. Still trembling in the bed at Lawrence Memorial, he looked up and told his mom and dad, “All I can do is go forward.” Susan ran through a mental checklist: Get Mike back into treatment; alert his caseworker; and figure out how to stop him from scoring another fix. But it was the weekend; time and resources weren’t on her side and Mike would soon be teetering toward a wrenching bout of dope sickness.